
(Viber, Whatsapp, Cell) +977 9851022814


Altitude sickness in Nepal is not something that only happens to the unprepared. Furthermore, it is not something fitness, experience, or expensive gear can guarantee you will avoid. Moreover, it is something that happens to humans — sometimes predictably, sometimes with no warning at all — and the numbers coming out of Nepal’s trekking regions deserve to be read clearly before anyone sets foot above 3,000 metres. Consequently, this blog is not here to frighten you off the mountains. It is here to make sure you come back from them.
Alliance Treks has been guiding high-altitude treks in Nepal for over 30 years. Our guides have handled everything from mild headaches at Namche to helicopter evacuations from the Larke La Pass. If you are planning a Nepal trekking trip above 3,500 metres, what follows is the most important preparation you will do.
Altitude sickness in Nepal is a common issue faced by trekkers and travelers who are not used to high-altitude climates and rapid elevation gain. As per the report published on Nepal Press, in the 2024–25 trekking season, 18 tourists died in Nepal from causes directly linked to altitude sickness and rapid ascent. Furthermore, those 18 people came from eight different countries including US, Germany, South Korea, Switzerland, India, and others. Moreover, they were not all unfit or inexperienced. They were trekkers who went up too fast, missed the early warning signs, or did not say anything until it was too late. Additionally, the Manang district alone recorded three altitude-related deaths in a single month in October 2025 near Yak Kharka and the Thorong La approach at 4,500 metres.
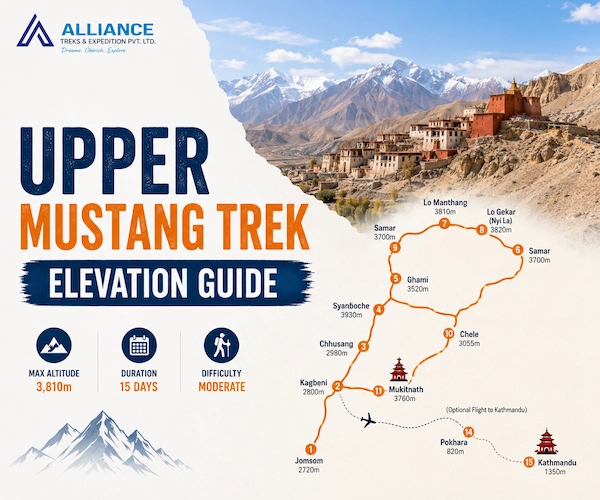
What makes altitude sickness in Nepal particularly dangerous right now is modern road infrastructure. Furthermore, improved jeep tracks now allow trekkers to reach elevations above 3,800 metres within hours of leaving Pokhara or Kathmandu and completely bypassing the gradual ascent that the body requires. Moreover, the Jomsom–Muktinath route has become a specific hotspot for rapid-ascent casualties because visitors can fly to Jomsom at 2,720 metres and reach Muktinath at 3,800 metres by jeep the same day. Consequently, altitude sickness in Nepal is increasingly a problem of infrastructure outpacing human physiology. Before heading above 3,500 metres, it is worth reading Alliance Treks’ complete guide to safe trekking in Nepal which covers everything from permit requirements to emergency protocols.
According to a 2022 research study on high-altitude illness conducted by the National Institutes of Health (NIH) and PMC in the Nepal Himalayas, oxygen levels at Everest Base Camp are nearly 50% lower than at sea level, while at the summit of Everest, they drop to around one-third.
The air at altitude contains the same percentage of oxygen as at sea level which is approximately 21 percent. Furthermore, what changes is barometric pressure: the air gets thinner, oxygen molecules spread further apart and each breath delivers fewer of them to your lungs. Moreover, the medical term for this is hypobaric hypoxia and it is the single underlying cause of every form of altitude sickness in Nepal from mild Accute Mountain Sickness (AMS) to fatal High-altitude pulmonary edema (HAPE) and High-Altitude Cerebral Edema (HACE). Additionally, during the Everest Base Camp Trek, the oxygen level at Everest Base Camp (5,364 meters) is only about half of what it is at sea level. At the summit of Everest, it drops even further to nearly one-third.
Your body responds immediately. Furthermore, breathing rate and heart rate increase. Over several days, kidneys adjust blood acidity to allow deeper breathing, and bone marrow ramps up red blood cell production. Moreover, this process — acclimatisation is genuinely remarkable. Consequently, the core rule of altitude safety is not complicated, simply give your body the time it needs. The problem is when you do not. When ascent outpaces adaptation, fluid leaks from blood vessels into surrounding tissue — producing, in mild cases, the headache and nausea of AMS and in serious cases, the fluid accumulation in lungs or brain that can kill within 24 hours.
Altitude sickness in Nepal presents in three distinct clinical forms and understanding the difference between them is one of the most important things you can do before any high-altitude trek. Furthermore, Acute Mountain Sickness — AMS which is common, manageable, and usually resolves with rest. Moreover, High Altitude Cerebral Edema (HACE) and High-Altitude Pulmonary Edema (HAPE) are medical emergencies that can move from early symptoms to fatal outcomes within hours. Additionally, a critical and frequently fatal error is treating HACE or HAPE symptoms as if they were ordinary AMS. Consequently, knowing which is which before you are at 4,500 metres in the dark is not optional knowledge. According to a research study on acute mountain sickness and high-altitude health risks published in PLOS Global Public Health, HACE and HAPE can develop from ordinary AMS within just a few hours. If any group member cannot walk in a straight line, appears confused, has blue lips, or is coughing frothy pink sputum, it should be treated as a medical emergency. Immediate descent is strongly recommended without waiting until morning.
| Type | Symptoms | What To Do |
|---|---|---|
| AMS (Mild) | Headache 6–12hrs after arrival, nausea, poor sleep, fatigue, dizziness. | Stop ascending. Rest. Hydrate. Ibuprofen for headache. Wait until fully resolved. |
| AMS (Severe) | Headache that does not respond to painkillers. Vomiting. Shortness of breath. | Descend 300–500m immediately. Do not sleep at the same altitude. |
| HACE | Cannot walk in a straight line. Confusion. Stumbling. Altered consciousness. | EMERGENCY. Descend NOW, even at night. Gamow bag. Immediate evacuation. |
| HAPE | Breathless at rest. Persistent cough. Frothy or pink-tinged sputum. Blue lips/nails. Gurgling lungs. | EMERGENCY. Descend immediately. Administer oxygen. Keep warm. Evacuate. Nifedipine if available. |
If you are unsure which Nepal trekking route is right for your fitness and altitude experience, Alliance Treks can help you choose one that builds acclimatisation in correctly from day one.
Every major altitude threshold on Nepal’s popular trekking routes, with documented AMS prevalence rates:
| Altitude | Risk Level | AMS Rate | What This Means |
|---|---|---|---|
| 2,500m | AMS begins | ~25% | First warning zone. Sensitive trekkers feel it here. |
| 3,000m | AMS common | Up to 75% | 3 in 4 people feel some symptoms. The real threshold. |
| 3,440m | High risk | 30–35% | Namche Bazaar — many trekkers underestimate this. |
| 4,130m | Very high risk | 34–57% | Annapurna Base Camp. Highest AMS band documented. |
| 4,500m | Serious risk | 40%+ | Thorong La approach. Near-universal mild symptoms. |
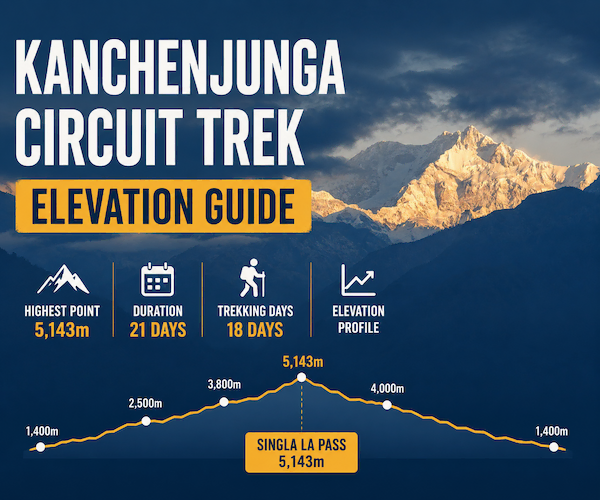
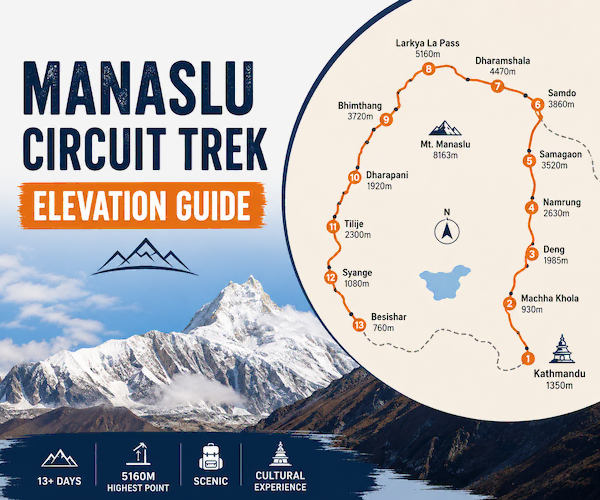
| 5,160m | Extreme | 50%+ | Larke La Pass, Manaslu Circuit. Guide monitoring essential. |
| 5,364m | Extreme | 50%+ | Everest Base Camp. Supplemental O₂ available at camp. |
According to AMS Prevalence Study, 25.78% AMS prevalence at Lobuche on the Everest Base Camp route from a survey of 2,983 trekkers across 91 countries — the largest AMS dataset ever published for Nepal.
Similarly, as per the study conducted on AMS in Annapurna region 34–57% — NIH / PMC, 34–57% AMS prevalence in the Annapurna trekking region documented across multiple peer-reviewed studies. On the worst days, more than half of trekkers are sick.
Trekkers on routes like the Everest Base Camp Trek and the Manaslu Circuit Trek pass through the highest-risk altitude bands. Alliance Treks builds mandatory acclimatisation days into both itineraries specifically because of these numbers.
Altitude sickness in Nepal has no correlation with physical fitness. Furthermore, the marathon runner and the office worker face essentially identical AMS risk at the same altitude with the same ascent rate. Moreover, your cardiovascular fitness affects how well you perform at altitude, not how well you acclimatise. Consequently, the fittest people on the trail are sometimes the most at risk — they feel strong, push harder, ascend faster, and ignore early warning signs.
Many trekkers assume that surviving altitude on a previous Nepal trek means they will be fine again. Furthermore, altitude tolerance varies significantly between trips for the same person depending on ascent rate, sleep quality, hydration, and recent illness. Moreover, there is documented genetic variation in altitude tolerance, but even that is not a reliable predictor from trip to trip. Consequently, Alliance Treks guides treat every group member as equally vulnerable regardless of their trekking history.
According to a 2025 PLOS Global Public Health research study on AMS symptom onset timelines, classic acute mountain sickness symptoms usually do not appear while trekking. Instead, they commonly develop six to twelve hours after reaching a higher altitude, often during sleep or early in the morning. Waking up with a headache, nausea, dizziness, or unusual exhaustion despite proper rest can be one of the earliest warning signs of AMS. This is why the first morning at a new altitude is considered the most critical time to monitor symptoms during a high-altitude trek.
Alcohol suppresses breathing rate during sleep, which is already compromised at altitude. Furthermore, it causes dehydration, which accelerates AMS symptoms. Moreover, even moderate consumption in the first 48 hours at a new altitude has been shown to increase AMS risk and severity. Consequently, Alliance Treks guides advise no alcohol for the first two nights at any significant altitude gain. This is not excessive caution. It is science.
Research published in PLOS Global Public Health in 2025 shows that High Altitude Pulmonary Edema (HAPE) does not always develop as a progression of Acute Mountain Sickness (AMS). It can occur independently, usually one to four days after reaching elevations above 2,500 meters. The study also notes that trekkers may feel relatively normal without headaches or typical AMS symptoms while HAPE develops silently. Early warning signs are often limited to increasing breathlessness and a persistent dry cough. Because of this, difficulty breathing while resting at high altitude should never be considered normal and must be reported immediately.
The treatment for serious altitude sickness is descent, and the response is often dramatic and fast. Furthermore, a trekker with early HACE symptoms who descends 300 to 500 metres will often show significant improvement within minutes, not hours. Moreover, the Gamow bag — a portable pressurisation device Alliance Treks carries on remote high-altitude routes — simulates descent by increasing pressure around the patient, buying time when immediate descent is not possible. Consequently, the altitude sickness rule that saves more lives than any other is simply: when in doubt, go down.
A 2025 report by Nepal News on increasing altitude sickness cases explains that improved jeep roads in Nepal’s trekking regions now allow travelers to reach elevations of nearly 3,800 meters within only a few hours from Pokhara, skipping the gradual acclimatization process entirely. The report also identified rapid road access as a contributing factor in several trekking deaths during the 2024–25 season. Likewise, trekkers flying directly to Lukla at 2,860 meters miss the slower altitude adjustment that earlier Jiri-to-Everest routes naturally provided.
Research on acute mountain sickness further shows that nearly 75% of people at around 3,000 meters experience at least mild AMS symptoms. This includes fit and experienced trekkers as well, showing that altitude affects people regardless of physical fitness or trekking experience.
Alliance Treks has built altitude safety into the operational framework of every high-altitude route we operate, refined over 30 years of Himalayan guiding. Furthermore, every guide carries a calibrated pulse oximeter and records group oxygen saturation readings every morning above 4,000 metres — tracking each person’s baseline and watching for drops that precede symptom onset. Moreover, all guides hold wilderness first aid certification with specific altitude medicine training including the Lake Louise Score, the HACE walking test, and the HAPE breath-sound assessment. Additionally, every group on routes above 4,500 metres carries supplemental oxygen and a Gamow bag.
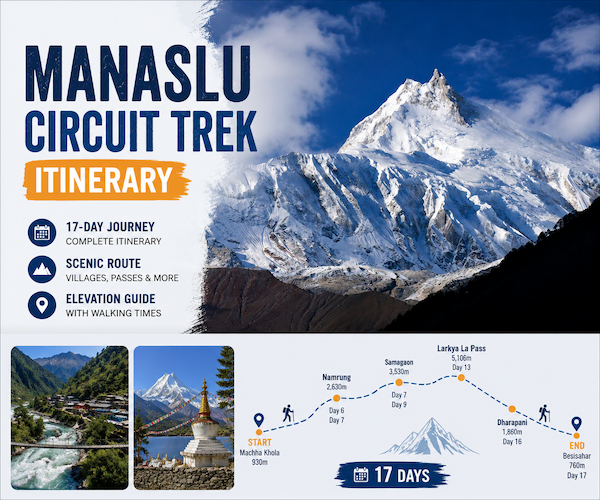
Our Manaslu Circuit Trek includes a mandatory acclimatisation day at Samagaon at 3,530 metres before the Larke La Pass crossing. Our Everest Base Camp Trek includes both the Namche and Dingboche rest days. Furthermore, if you see a competitor’s itinerary that reaches those altitudes faster than ours, that speed is not an advantage. It is a risk compression that the altitude data does not support.
No. Furthermore, Diamox speeds up acclimatisation and reduces AMS symptoms but it is not a substitute for slow ascent. Moreover, trekkers who take Diamox and ascend too fast can still develop serious altitude sickness. Consequently, it is a support tool, not a safety net. Always use it alongside correct acclimatisation planning, not instead of it.
At sea level, healthy saturation is 95 to 100 percent. Furthermore, at 3,500 to 4,500 metres, readings of 85 to 95 percent are typical and not necessarily concerning. Moreover, readings below 80 percent warrant active monitoring and rest. Additionally, rapid drops between daily readings — even if the absolute number is still above 80 — can signal developing altitude sickness before symptoms appear. Consequently, the morning pulse oximeter reading is one of the most valuable tools an Alliance Treks guide uses.
Research does not consistently show that older trekkers face greater AMS risk than younger ones. Furthermore, younger trekkers may actually be at higher risk because they are more likely to ascend aggressively and less likely to report symptoms. Moreover, the genuine predictors of AMS risk are previous AMS history, ascent rate, and individual physiology — none reliably age-dependent. Consequently, age alone is not a reason to avoid high-altitude trekking in Nepal.
Standard policies vary significantly. Furthermore, helicopter evacuation from high altitude in Nepal costs between USD 3,000 and USD 10,000 or more. Moreover, many standard policies cut off at 4,000 or 5,000 metres. Consequently, confirm explicitly that your policy covers trekking at your target altitude and includes emergency medical evacuation before booking any Nepal trek above 3,500 metres. Alliance Treks makes this a non-negotiable pre-departure requirement for every client.
Tell your guide immediately and without softening the description. Furthermore, do not let your partner downplay symptoms and do not let schedule pressure influence the decision to descend. Moreover, for any symptoms suggesting HACE or HAPE — confusion, breathlessness at rest, inability to walk straight, blue lips — the only correct action is immediate descent. Consequently, the most important thing you can do for a symptomatic trekking partner is override their protests and get them lower.
Altitude sickness in Nepal is real, it is documented and it kills people every year. Furthermore, the vast majority of those deaths were preventable. Moreover, the science is not complicated and the rules for avoiding serious altitude sickness are not onerous — they simply require discipline, honesty, and the judgment to choose a trekking company that builds safety into its itineraries rather than cutting corners to save days. Additionally, Alliance Treks has been guiding trekkers safely through Nepal’s high-altitude routes for over 30 years and our record speaks for itself. Consequently, if you are going high in Nepal, go prepared and go with people who know what they are doing.
Trek safely with Alliance Treks.





Alliance Treks & Expedition Pvt. Ltd. Once is not enough for naturally and culturally Himalayas